SCOPE | Provider Update
September 2023
Clinical Matters
USPSTF releases updated recommendations for colorectal cancer screenings
Revisions based on evidence that screening should begin at age 45; several different methods can accurately detect early-stage cancer and adenomatous polyps.
According to the American Cancer Society, colorectal cancer is the third leading cause of cancer death for both men and women, with an estimated 52,550 individuals in the United States (US) projected to die of colorectal cancer in 2023.1 In May 2021, the United States Preventive Services Task Force (USPSTF) updated its recommendation to screen for colorectal cancer in adults starting at age 45, an update from the 2016 recommendation to screen adults ages 50-75 years old.
The USPSTF found adequate evidence that screening at average risk for colorectal cancer with several different methods can accurately detect early-stage colorectal cancer and adenomatous polyps.
Start the conversation with your patients early, since early detection and screening can save lives.
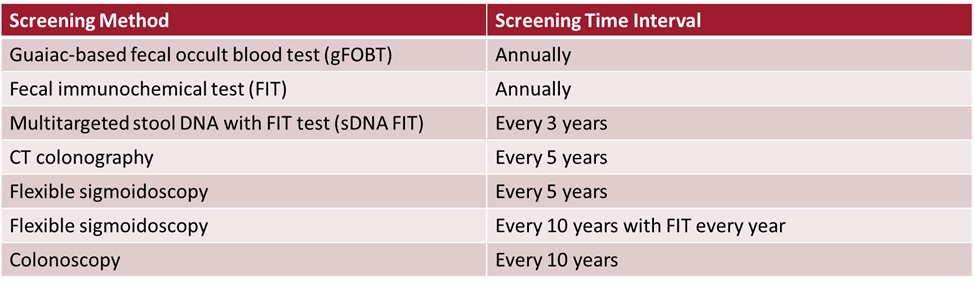
There are several screening options available to your patients, based on individual risk factors (e.g., age, other chronic conditions, patients’ fear of completing the screening, etc.). The table below outlines the applicable screening methods for members at average risk. Those at increased risk may have different recommendations.
Making clear recommendations to patients and emphasizing the importance of screening and prevention can help improve outcomes. Asking patients about their specific questions, concerns, and preferences can help patients select a screening method that meets their needs.
As a reminder, also noted in the final USPSTF recommendation, a positive non-invasive stool-based screening test (e.g., FIT, FOBT, and fecal DNA) or direct visualization test (e.g., sigmoidoscopy or CT colonography), should initiate a follow-up colonoscopy for comprehensive and complete screening practices.
Follow-up colonoscopy after a positive non-invasive stool-based screening test or direct visualization screening test is therefore required to be covered without cost sharing.
For Commercial and State members in the age range of 45-75 years, and Medicare members in the age range of 45-85 years with a positive stool-based colorectal cancer screening test or direct visualization screening test, the follow-up colonoscopy should be included in the preventive care service.
Outreach calls to members who should be screened
To help close gaps in members’ care, Independent Health partners with providers to make reminder calls for their patients who appear to be overdue for a colorectal cancer screening. The telephonic outreach campaign targets Commercial, Medicare, and Medicaid members, and aims to engage members who appear in need of colorectal cancer screening.
The purpose of the call is to educate members on the importance of colon cancer screening, discuss any member barriers to screening, and support the member to move forward on screening orders received from their provider. Members that do not have an order for a colon cancer screening test will be encouraged to reach out to their provider to discuss screening options.
Member Incentives:
Members may be eligible to earn an incentive for completing a colorectal cancer screening based on their benefit plan:
- Medicare members may earn $10 in rewards toward their NationsOTC® account for getting screened for colon cancer.
- Commercial Insured and Commercial Self-funded may earn $10 for getting screened for colon cancer. RedShirt Rewards allows members to earn up to $30 each plan year in the form of gift cards to retailers of their choice.
Provider Incentives:
Providers who participate with Independent Health's Primary Value Program, the Medicaid Provider Incentive Program, and/or are part of an existing IPA, are incentivized to close members colorectal cancer screening gaps in care.
- 2023 Primary Value Program: Primary Care is a value-based reimbursement program that began in 2018. This program rewards primary care physicians for providing value by focusing on quality measures, and closing gaps in care, across the Commercial, Medicare, and Medicaid lines of business.
- 2023 Medicaid Provider Incentive Program: This quality incentive program is designed to improve the overall quality of care for Independent Health’s MediSource, MediSource Connect and Child Health Plus members by providing incentives to primary care physicians support increased delivery of recommended care for patients attributed to their practice. Log into your portal account to view the 2023 Medicaid Provider Incentive Program Guide.
If you would like to learn more about participating in the programs mentioned above, or have any questions, please contact Independent Health’s Provider Relations department by phone at (716) 631-3282 or 1-800-736-5771, Monday through Friday from 8 a.m. to 6 p.m. or reach out by email at Engagement@independenthealth.com.
References:
American Cancer Society. (2023, January 13). Key Statistics for Colorectal Cancer. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html#:~:text=In%20the%20United%20States%2C%20colorectal,about%2052%2C550%20deaths%20during%202023.
United States Preventive Services Task Force. (2021, May 18). Final Recommendation Statement Colorectal Cancer: Screening. Recommendation: Colorectal Cancer: Screening | United States Preventive Services Taskforce (uspreventiveservicestaskforce.org)
How to help curb antibiotic resistance
Overuse and misuse of antibiotics encourage the development of antibiotic-resistant bacteria. This article includes easy ways to help maintain the efficacy of antibiotics.
The Centers for Disease Control and Prevention (CDC) estimates that in the United States antibiotic-resistant bacteria cause over 2.8 million illnesses and more than 35,000 deaths each year. Additionally, antibiotic resistance has a national cost of $4.6 billion annually.
The primary drivers of antibiotic resistance are overuse and misuse. The CDC estimates 28% of antibiotics prescriptions written were unnecessary. Of the necessary antibiotic prescriptions written, 50% included inappropriate antibiotic selection, dosage, and duration of use.
To help curb the rate of antibiotic resistance, follow these educational and counseling tips:
- Prevent infections: Everyone has a role to play in preventing infections.
- Keep your hands clean. Counsel patients on proper hand washing technique and explain how this fights germs.
- Get vaccinated. Encourage age- and risk-appropriate vaccinations for flu, COVID, RSV, and pneumonia.
- Watchful waiting. Two out of three children with otitis media will recover without antibiotics.
- The American Academy of Family Physicians (AAFP) recommends not using antibiotics in children ages 2 to 12 years with non-severe symptoms unless symptoms persist for more than 48 to 72 hours.
- Viral infections: antibiotics are not indicated for viral infections.
- Acute bronchitis is caused by a virus in approximately 95% of cases.
- Upper respiratory tract infections are most commonly caused by viruses.
- Pharyngitis is caused by a virus in approximately 50% to 80% of cases.
- The common cold and flu, both caused by viruses, are easily confused. Help patients differentiate between them.
- If a patient has the flu, an anti-viral is most effective if used within 48 hours of illness onset. These include oseltamivir (Tamiflu), zanamivir (Relenza) or baloxavir marboxil (Xofluza). Prevention is the best approach. Encourage patients to receive their annual flu shot.
- Steptococcal pharyngitis: symptoms overlap with other diseases.
- According to the AAFP guidelines, a diagnosis of steptococcal pharyngitis requires a positive test for group A Streptococcus prior to treatment.
- Empiric treatment with an antibiotic may be used with a Centor Score* of 3 or higher or with a positive rapid test result.
- Improper use. If an antibiotic is required, inadequate doses or ending treatment early may lead to resistance.
- Counsel patients to take the full dose of their antibiotic for the duration prescribed.
To help start a conversation with your patients, consider displaying commitments in support of antibiotic stewardship in your office. Poster-size commitment letters in examination rooms can help reduce inappropriate antibiotic prescribing, which can positively affect some HEDIS quality measures. You can download posters and view other resources on the CDC's Appropriate Antibiotics Use website, the NYS Department of Health's Antibiotic Resistance website and the Choosing Wisely website.
*Centor Score: A tool to help determine which patients need no testing, a throat culture or rapid antigen test, or empiric antibiotic treatment. The score is based on a patient’s symptoms (cough, swollen/tender cervical nodes, temperature, swollen tonsils/exudate) and age. Additional factors (e.g., a recent contact with a known group A streptococcal infection) may also be considered when determining the need for antibiotic treatment. Choby BA. Diagnosis and Treatment of Streptococcal Pharyngitis. Am Fam Phys. 2009;79(5):383-390
References:
Centers for Disease Control and Prevention, Antibiotic Resistance Threats in the United States, 2019. Atlanta, GA: U.S. Department of Health and Human Services, CDC; 2019.
Nelson RE et al, National Estimates of Healthcare Costs Associated With Multidrug-Resistant Bacterial Infections Among Hospitalized Patients in the United States, Clin Inf Dis. 2021;72(S1):S17-S26.
Hersh AL et al. Unnecessary Antibiotic Prescribing in US Ambulatory Care Settings, 2010-2015. Clin Inf Dis. 2021;72(1):133-137.
Centers for Disease Control and Prevention (CDC). Office-related antibiotic prescribing for persons aged ≤14 years — United States, 1993—1994 to 2007—2008. MMWR Morb Mortal Wkly Rep. 2011;60(34):1153-6.
Pichichero ME. Dynamics of Antibiotic Prescribing for Children. JAMA. June 19, 2002;287(23):3133-5.
Shapiro DJ et al. Antibiotic Prescribing for Adults in Ambulatory Care in the USA, 2007–09. J Antimicrob Chemother. 2014;69(1):234-40.
Singh A et al. Acute Bronchitis. National Heart, Lung and Blood Institute. Reviewed July 2023.
Thomas M et al. National Library of Medicine. StatPearls. Upper respiratory tract infection. 2021.
Wolford RW et al. Pharyngitis. National Heart, Lung and Blood Institute. Updated May 2023.
Asthma Rescue/Reliever Medication Math: The Rules of Two
The "Rules of Two" is a simple way to determine whether a patient's asthma symptoms are under control.
The “Rules of Two”, often used as a simple way to monitor asthma control, suggest that using albuterol more than two times weekly might indicate that your patient’s asthma symptoms are not well controlled.
We can take the concept behind the “Rules of Two” and use some basic math to identify patients who may benefit from a different approach to managing their asthma.
Each albuterol rescue/reliever canister contains 200 actuations (or “puffs”). Typical instructions on an albuterol prescription state “Take 2 puffs every 4 to 6 hours as needed for wheezing or trouble breathing.” That’s 100 doses per canister (200 actuations divided by 2 puffs).
Since there are 52 weeks in a year, 2 doses x 52 weeks = 104 doses annually. That means patients with well-controlled asthma would only need to fill their prescription once or twice a year. More than 104 doses annually would suggest your patient needs further medical treatment for their asthma symptoms.
With many patients filling six to twelve albuterol inhaler prescriptions a year (equaling 600 to 1200 doses annually of albuterol for a year which contains only 365 days), there are opportunities to optimize controller regimens, reducing their reliance on albuterol rescue inhalers.
Why does this matter?
Evidence suggests that overreliance on albuterol rescue for asthma management leads to poorer outcomes, including greater risks of hospitalization and death due to asthma exacerbations.
The Asthma Medication Ratio (AMR) HEDIS measure looks at the ratio of the number of your patient’s total asthma medication (both controller and rescue) to the number of rescue medications used. If the patient’s ratio is <0.5 (more relievers than controllers used), these patients will count against you in that year’s measure.
A patient will fall into the measure’s denominator if:
- They have two or more outpatient visits coded with an asthma diagnosis; or,
- One or more hospital visits coded with an asthma diagnosis; or
- They fill four or more asthma medications (both rescue and controller medicines)
The best way to meet the measure is to reduce albuterol refills and increase controller medication refills.
What you can do:
- Write for fewer refills. Patients typically fill all refills, even if they don’t need to.
- Work with patients using more than two albuterol a year to optimize their asthma management.
- Look at other options if your patient doesn’t like their current asthma controller medication.
CDC urges early recognition, prompt treatment of sepsis
Helpful guides from the CDC are available to increase awareness of and prevent sepsis
An online resource page called Get Ahead of Sepsis from the Centers for Disease Control and Prevention (CDC) urges healthcare professionals, patients, and caregivers to be alert to the signs and symptoms of sepsis, act fast if sepsis is suspected, and prevent infections that can lead to sepsis. Sepsis affects at least 1.7 million adults in the US. Without fast recognition and treatment, many patients will die.
Office Matters
Coming later this year: New Member ID Numbers
Self-funded and commercial members will be assigned new ID numbers that begin with W.
Recently Independent Health announced that we will offer an expanded, comprehensive national network for our commercial and self-funded lines of business this fall.
The enhanced national network will cover members who live outside of Independent Health’s traditional Western New York service area, while serving as the travel network for members who live locally.
To accommodate the national network, all Independent Health commercial and self-funded members will receive new ID cards with new ID numbers upon their plans’ renewal dates. The new ID numbers will begin with “W.” (The ID numbers for Medicare and State program members will not change).
It is important to ask patients if they have new ID cards and to use their new Member ID numbers. However, this should have no effect on your billing, as the new ID number will track to the member’s current ID number.
Timing:
- A limited number of self-funded members will get their ID cards before December 1.
- Starting in December, commercial group members with a January 1 renewal date will begin receiving their new ID cards in December. Members may begin using their new ID cards as soon as they receive them.
Upcoming member campaigns to encourage our members to take greater control of their health
Throughout the year, the Health Care Services and Population Health Management Departments deploy various tactics to encourage members to take a more active role in their health.
During the month of September, Independent Health will be conducting the following member engagement/outreach campaigns:
Colorectal Cancer Screening Reminder
This telephonic outreach campaign will engage members who are overdue for a colorectal cancer screening. The purpose of the call is to provide education around the importance of colon cancer screening, address member barriers to screening, and encourage the member to follow through on screening orders received from their provider. Members that do not have an order for a colon cancer screening test will be encouraged to have a conversation with their provider regarding screening.
- Outreach method: Outbound telephone call campaign
- Target members: Medicare and Medicaid members who are overdue for a colorectal cancer screening
- Timeframe: September 2023
Social Determinants of Health Screening
This telephonic outreach campaign will engage Essential Plan members in a conversation around screening for social determinants of health to identify any needs the member has for things such as food, housing, and transportation. If a need is identified, Independent Health will assist the member in making a connection to a community resource to address the need.
- Outreach method: Outbound telephone call campaign
- Target members: Essential Plan members
- Timeframe: September 2023
Breast Cancer Screening Reminder Campaign
This campaign will target women ages 50 to 74 within the Medicaid line of business who are overdue for a mammogram. The goal of this telephonic outreach campaign is to maximize mammography participation. Education around the benefits of receiving a mammogram, as well as information regarding how to address any barriers, and how to follow through with their provider’s orders will be discussed. Members that do not have an order for a mammogram will be encouraged to have a conversation with their provider.
- Outreach method: Outbound telephone call campaign
- Target members: Women ages 50 to 74 who are overdue for a mammogram- Medicaid members only
- Timeframe: September 2023
Educating patients with asthma
Asthma is the most common condition among our commercial and Medicaid populations from children to young adults. In Western New York, over 1.2 million adults were estimated to have asthma in 2021; from 2018-2020, children aged 0-17 years accounted for over 5,000 emergency room visits related to asthma. Nationally, asthma causes almost 10 deaths per day, with Black Americans being 2 to 3 times more at risk than any other racial or ethnic group.
Starting in September, Independent Health will send eblasts to members regarding asthma and asthma management. The three eblasts include:
- Asthma Action Plans
- Coordinating Your Child’s Care between the school nurse and children’s providers to better manage triggers, symptoms, and rescue therapy during school hours.
- Trigger Identification and Management
These eblasts have three objectives:
- Patient self-advocacy and self-management strategies for their asthma, including trigger identification and management
- Helping patients understand the roles of controller and rescue medications and when to use them to improve asthma outcomes
- Optimizing the care relationship between school nurses and primary care providers for school age children
Target members: Members age 18 to 64 with a diagnosis of asthma; E-mail #2 is targeted to the guardians of members aged 5 to 18 with a diagnosis of asthma.
Timeframe: one informational eblast from this series will go out each month from August through October.
Pharmacy Updates
Formulary and Policy Changes
The following documents are available in PDF. We encourage you to open and download them, as they contain important information and updates:
- Medicare Advantage formulary changes for individual and group members effective Sept. 1, 2023.
- Pharmacy Benefit Dimensions 5-Tier formulary changes effective Sept. 1, 2023.
- Pharmacy Benefit Dimensions 3-Tier formulary changes effective Sept. 1, 2023.
View the most up to date versions of Independent Health’s policies when logged in to our provider portal
Magellan Rx, administered by Magellan Rx Management, reviews select specialty drug prior authorization requests on Independent Health’s behalf.
Independent Health's drug formulary
Access Independent Health's drug formulary here.
To obtain a hard copy, please contact Independent Health Provider Relations by calling (716) 631-3282 or 1-800-736-5771, Monday through Friday from 8 a.m. to 6 p.m.
In the News
Independent Health in the News
Fitness in the Parks fosters friendships, healthy habits, Healthy Vision blog, Aug. 16, 2023
How to step up your walking routine, Healthy Vision blog, Aug. 1, 2023
Spotlight
Top Takeaways this Month
September 2023 Policy Updates: View them here
Primary Care Physicians: Free CME-eligible webinar Sept. 13: Pratibha Bansal, M.D., DABA, FIPP, will present "Practical tools for primary care physicians to treat myofascial pain. Register here
Office Matters Webinar for Primary Care Physicians: Looking Ahead to 2024. Mark your calendars for Sept. 26 at 7:30 a.m. Watch your secure message inbox for registration details coming soon!
Annual Training: Did you and your staff complete your annual required compliance training modules? More information.
Updated Provider Manual: We have updated the Provider Manual. It's posted in the secure portal. Log in to view.
Update your Digital Contact Information: Federal & State regulations require practices to provide specific information. Learn more here.