SCOPE | Provider Update
December 2023
Clinical Matters
Screening & referring Independent Health members for behavioral health & health-related needs
Primary care providers are in a unique position to be able to screen, diagnose, and treat a range of behavioral health issues; this article discusses the screening tools that can help.
Primary care providers are often the first point of contact for patients looking to receive care from a specialist, including Behavioral Health (BH) providers.
Evidence shows that people who have regular access to primary care live longer, feel better, and avoid disability and long absences from work. Primary care offices are in a unique position to be able to screen, diagnose, and treat a range of behavioral health issues, such as depression, anxiety, and substance use. Patients who are not adequately treated for these concerns are less likely to obtain the necessary treatment and medications which could lead to sub-optimal health.
Best practice is for all office team members including social workers, nurses, and physicians to have knowledge of and the ability to perform BH and Social Determinant of Health (SDOH) screenings on every patient. Major life events, such as job loss, pregnancy, or death of a family member can trigger symptoms. When staff are professionally trained and prepared to have these discussions, patients will feel supported and comfortable sharing these symptoms and life events.
Examples of Screening Tools
Social Determinants of Health (SDOH)
- Protocol for Responding to & Assessing Patients’ Assets, Risks & Experiences (PRAPARE)
- Accountable Health Communities Health-Related Social Needs Screening Tool (AHCM)
- HealthLeads
Depression/Anxiety
- Patient Health Questionnaire (PHQ-9)
- Generalized Anxiety Disorder Screener (GAD-7)
Substance Use Disorder
- Alcohol Use Disorders Identification Test (Audit-C)
- Cut, Annoyed, Guilty, and Eye - Adapted to Include Drugs (CAGE-AID)
- Screening, Brief Intervention, and referral to Treatment (SBIRT)
Implementing routine screenings on all patients, new and current, may allow practice to identify areas where assistance is needed.
Once a screening is complete, staff should be prepared to assist patients with the next steps, including a warm hand off to an internal behavioral health specialist, or making a referral to a specialty care provider.
Primary care office staff can contact the patient’s insurance company to obtain behavioral health providers who are in network. Coordination between primary care providers and behavioral health specialists is paramount to the success of treatment and coordination of care, to ensure metabolic screenings occur for patients prescribed antipsychotic and/or ADHD (attention deficit hyperactivity disorder) medications. SDOH factors can impact whether a patient will attend and continue with appointments.
If you believe that you or your staff could benefit from training and/or resources on using SDOH/BH screenings, or finding available resources for members, please see the below resources:
- Erie County Dept. of Health –Mental Health First Aid (MHFA) training. Call 716-858-2385, email at healthequity@erie.gov
- Project Teach – Helps pediatric primary care providers, OB/GYNs, and other primary care clinicians treating women with maternal mental health concerns. Call 855-227-7272 or visit projectteachny.org.
- SAMHSA – Provides Crisis line access, treatment location assistance, research, resources for caregivers and the community, as well as training for providers. Individuals may call its 24-hour confidential helpline for assistance with referrals and information about mental health and substance use disorders at 1-800-662-HELP (4357); Email: SAMHSAInfo@samhsa.gov or visit samhsa.gov.
- National Institute on Drug Abuse – Provides information on current research, training, resources (including screening tools), and available grants/funding. Visit nida.nih.gov for more information, and view screening tools here.
- 211 WNY – Community Resource Specialists who cover seven counties in WNY: Cattaraugus, Chautauqua, Erie, Genesee, Niagara, Orleans, and Wyoming. For more information, call 211 (or 888-696-9211); or visit 211wny.org.
- Independent Health – Member Services Department at 716-250-7183 or 1-888-891-9372 (TTY:711), Monday through Friday at 8 a.m. to 8 p.m. Case Management services are also available.
References
Abrams, M. (2013). Primary Care: Our First Line of Defense. The Commonwealth Fund – Health Reform & You.
Brown JD, Wissow LS, Cook BL, Longway S, Caffery E, Pefaure C. (2013). Mental health communications skills training for medical assistants in pediatric primary care. J Behav Health Serv Res. 40(1):20-35. doi: 10.1007/s11414-012-9292-0.
Drake, E. and Valenstein, M. (2021). Behavioral Health Integration into Primary Care. American Medical Association. Steps Forward.
Moen M, Storr C, German D, Friedmann E, Johantgen M. (2020). A Review of Tools to Screen for Social Determinants of Health in the United States: A Practice Brief. Population Health Management. (6):422-429. doi: 10.1089/pop.2019.0158.
Turner N. (2023). Family physicians: first point of contact, last line of defense. Can Fam Physician. 69(7):490-491. doi: 10.46747/cfp.6907490.
Follow-up care after mental illness or substance use disorder hospitalizations help prevent readmissions and relapse
Regular patient visits help providers detect early reactions to medications or other issues and can help prevent readmission.
Individuals who have been hospitalized for mental health and/or substance use disorders are at higher risk for symptom decompensation, hospital readmission, homelessness, violent behavior, suicide, and premature mortality. It is important that patients receive appropriate care after hospitalization, including an initial provider visit for assessment, and when needed, additional regular follow-ups. This is recommended to ensure that the patient has the proper support for the transition to home, school, and/or work environment, and do not lose any gains made during their hospitalization. When patients have regular visits, their providers can detect early reactions to medications or other issues that may arise, which can help prevent readmission. There are two measures in the HEDIS manual that help lay out best practices for these patients.
- Follow-up after Hospitalization for Mental Illness (FUH) - Patients who are six years of age or older and have been hospitalized for select mental health disorders or intentional self-harm should have an initial visit within 7 days after their discharge from the hospital. These visits can be provided through telehealth when appropriate; however, they must be facilitated by a mental health provider as described in the HEDIS Manual.
- Follow-up after High-Intensity Care for Substance Abuse (FUI) – Patients who are 13 years of age or older and have been hospitalized, placed in residential treatment, or detoxification for a diagnosis of substance abuse disorder should have an initial visit within 7 days after their discharge. These visits can be provided through telehealth when appropriate and can be facilitated by primary care providers.
It is important that practices receive timely alerts from hospitals for their patients and can sign up for systems such as HEALTHeLINK to assist. While hospitals and other inpatient facilities should schedule appointments for patients prior to discharge, it does not always happen. Practices should implement transition-of-care teams or transition-of-care processes to ensure timely follow up with newly discharged patients to assist with linkage to any services needed. Health care providers should establish processes generate appointment reminders and/or “reschedule” phone calls, texts, or mailings to patients if the patient misses or cancels a follow-up visit. Offering initial visits as telehealth appointments when patients are not able to make it into the office because of transportation or other responsibilities can ensure the patients are still assessed for needs and can prevent readmissions, allowing for a second in-person appointment to be scheduled at a later time.
For additional information on billing or coding, please reference the HEDIS manual.
Statins as a standard of care for diabetes and ASCVD
Primary care physicians should follow these recommendations, which align with Primary Value scorecard measures.
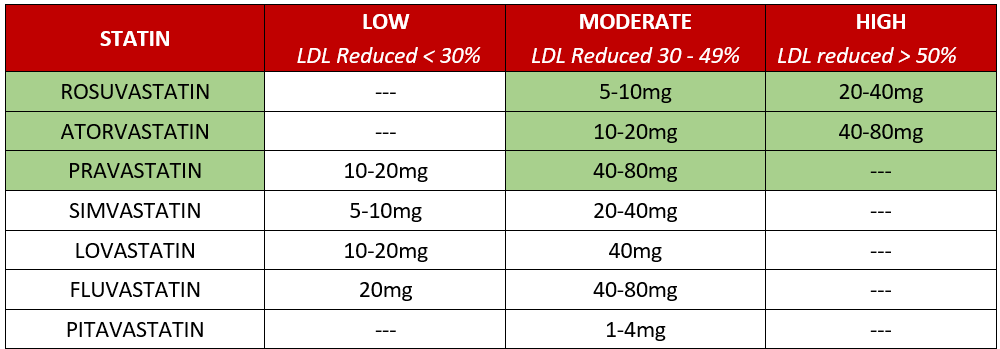
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of morbidity and mortality in high-income countries. Statins are the drug of choice and remain one of the most used and effective drugs for reducing LDL cholesterol, the risk of mortality and coronary artery disease in high-risk groups. Because of this known benefit, the following guidelines are part of Primary Value scorecard measures which align with HEDIS and STAR quality metrics
The Primary Value Scorecard measures recommend:
- All patients with ASCVD regardless of lipid levels receive moderate to high intensity statins for secondary prevention.
- All patients aged 40-75 with diabetes regardless of lipid levels receive moderate to high intensity statins.
ASCVD includes having a history of MI, CABG, PCI or other revascularization procedures, or a diagnosis of ischemic vascular disease such as angina, atherosclerosis of an extremity, or stroke.
To assess patients for statin use, we recommend reviewing each patient’s medical record, and:
- Prescribe a moderate to high intensity statin and send a new prescription to the patient’s pharmacy.
- For any patients that have had myalgia in the past, often a retrial with a different drug or a lower dose is tolerated. Retrial with a different drug is recommended annually. If the patient continues to experience myalgia after retrial, then code appropriately.
- If the patient has tried multiple statins & cannot tolerate due to muscle pains, the patient should be assessed and coded appropriately at next visit.
At the least, a moderate intensity statin is recommended for patients with ASCVD or diabetes. Statins are generally well tolerated, however statin-associated muscle symptoms are the most common side effect associated with treatment discontinuation. It is common to experience muscle pain from one statin, and not from another. For patients that have muscle pain and symptoms, try switching to another statin such as rosuvastatin, and pravastatin. Both rosuvastatin and pravastatin are less likely to cause myalgia/myopathy and are also a zero copay or very inexpensive for most patients.
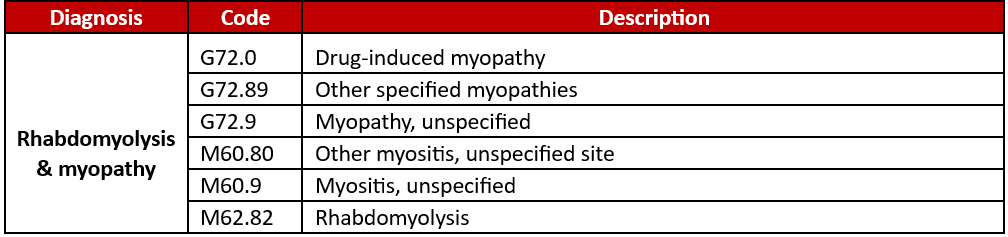
MYOPATHY EXCLUSION CODES
Patients who are intolerant to MULTIPLE statins & have a diagnosis of the following coded within the calendar year are excluded from this quality metric:
It’s important to review patient-level factors that may influence the decision to start statin therapy.
Help keep your patients informed & healthy by educating them on the benefits of statin therapy & prescribing statin therapy for them today. Independent Health supports your efforts to deliver quality, efficient care.
If you have any questions call our team of pharmacists at (716) 250-4480 or 1-844-808-1254, Monday through Friday from 8:30 a.m. to 4:30 p.m.
Office Matters
NYSDOH advises RSV vaccinations during 32 through 36 weeks of pregnancy
New statewide standing order allows pharmacies to administer the immunization.
The New York State Department of Health (DOH) recently shared updated information from the Centers for Disease Control and Prevention (CDC) regarding the RSV Immunization, BeyfortusTM (nirsevimab). The CDC advised that there is limited availability of nirsevimab, the long-acting monoclonal antibody immunization recommended for the prevention of RSV-associated lower respiratory tract infection in infants. You can read the full CDC advisory here. In response to the anticipated nirsevimab shortage, DOH advises administering a single dose of Pfizer’s bivalent RSVpreF vaccine (Abrysvo) during weeks 32 through 36 of pregnancy. Administering the vaccine to this population of pregnant people will provide newborns with protection from RSV-associated lower respiratory tract infection.
What you need to do
If your office is unable to administer Abrysvo to the pregnant member, a pharmacy may be able to. A new statewide standing order allows pharmacies to administer the immunization to pregnant people during weeks 32 through 36 of their pregnancy. Pharmacies with Medical Directors (typically chains) may have their own standing order. Pharmacies not using the statewide standing order may not be able to administer Abrysvo. To avoid any delay, contact the pharmacy to verify if they can administer Abrysvo under their standing order or provide a patient specific prescription.
For questions on RSV vaccine coverage, please call Independent Health’s Pharmacy Services Department at (716) 631-2934 or 1-800-247-1466, Monday through Friday from 8 a.m. to 5 p.m.
Final date to submit gaps-in-care corrections: Jan. 3, 2024
Make sure to get your gaps-in-care corrections into Independent Health if you find inaccuracies for certain reasons.
The last day to submit 2023 gap-in-care corrections for medical record documentation to Independent Health through our provider portal is Wednesday, January 3, 2024 at 6 p.m.
After this date, we will no longer accept gap-in-care corrections for the 2023 calendar year.
We will inform participating providers when we will begin accepting gap-in-care corrections for 2024.
The Gaps in Care Correction process allows for medical record documentation to be submitted to “correct” inaccuracies in quality measure results due to a variety of reasons, including:
- Encounters or lab values not available to the health plan
- Exclusions from a historical event (e.g., mastectomy)
- Service that was rendered under a different payer
If the correction is accepted, it will be reflected in an update to your quality rates (and Independent Health's), which allows for:
- A more accurate depiction of the quality of care that was rendered
- More accurate quality program reporting
- More targeted quality improvement effort
View the Gaps in Care Correction Process User Guide, view a webinar and learn more about submitting correction requests in our secure provider portal . (This information is in the Quality section under the Resources tab selection.)
If you have questions about the gaps in care correction process, performance reports or anything related to our provider portal:
Contact your Independent Health Physician Engagement Specialist or Email ProviderPortal@independenthealth.com
Coming later this year: New Member ID Numbers
Self-funded and commercial members will be assigned new ID numbers that begin with W.
All Independent Health commercial and self-funded members will receive new ID cards with new ID numbers upon their plans’ renewal dates. The new ID numbers will begin with “W.” (The ID numbers for Medicare and State program members will not change).
It is important to ask patients if they have new ID cards and to use their new Member ID numbers. However, this should have no effect on your billing, as the new ID number will track to the member’s current ID number.
Timing:
- A limited number of self-funded members have received their ID cards.
- Starting the month of December, commercial group members with a January 1 renewal date will begin receiving their new ID cards in December. Members may begin using their new ID cards as soon as they receive them.
Upcoming member campaigns to encourage our members to take greater control of their health
Throughout the year, the Health Care Services and Population Health Management Departments deploy various tactics to encourage members to take a more active role in their health.
During the month of December, Independent Health will be conducting the following member engagement/outreach campaigns:
Social Determinants of Health Screening
This telephonic outreach campaign will engage commercial members with non-emergent ED visits in a conversation around screening for social determinants of health to identify any needs the member has for things such as food, housing, and transportation. If a social need is identified, Independent Health will assist the member in making a connection to a community resource to address the need.
- Outreach method: Outbound telephone call campaign
- Target members: Targeted commercial members
- Timeframe: December 2023 to February 2024
Pharmacy Updates
Formulary and Policy Changes
Fourth quarter changes are available for review in PDF. We encourage you to open and download them, as they contain important information and updates:
Magellan Rx, administered by Magellan Rx Management, reviews select specialty drug prior authorization requests on Independent Health’s behalf.
Independent Health's drug formulary
Access Independent Health's drug formulary here.
To obtain a hard copy, please contact Independent Health Provider Relations by calling (716) 631-3282 or 1-800-736-5771, Monday through Friday from 8 a.m. to 6 p.m.
In the News
Independent Health in the News
This Buffalo nurse practitioner still makes house calls, bringing care to some of Buffalo Niagara's hard-to-reach patients - Buffalo News, Nov. 9, 2023 (Subscription required)
U.S. News & World Report Recognizes Independent Health's Medicare Advantage Plans - News release, Nov. 13, 2023
Spotlight
Top Takeaways this Month
December 2023 Policy Updates: View them here
Update your Digital Contact Information: Federal & State regulations require practices to provide specific information. Learn more here.
Time is Running Out #1: Complete your FWA/Cultural Competency Attestations: Learn more here
Time is Running Out #2: Gaps-in-Care Corrections deadline is Jan. 3, 2024. View details in Quality under the Resources tab in your portal account.